A Brief History of Public Health Education Accreditation
… and the unique contribution of ICAPHE
As of the 11th January 2026, accreditation of public health education is 80 years old [1],[2]. It first emerged in America, due to a combination of factors unique to the American system.
The first efforts to accredit public health education were an indirect result of attempts to standardise the sector in America. Established in 1920, the American Public Health Association’s (APHA) “Committee for standardisation” was headed by William Shepard who stated that “public health has become a profession” and accreditation would protect against “pseudo-trained people.”[3] These conditions were reflected also in American medical education. As noted in the Flexner report in 1910, “the (medical) schools were essentially private ventures, money-making in spirit and object”[4] with the result of an “over-production of ill trained men.” (sic)[5]. As a result, Flexner concluded that the number of U.S. medical schools could, in principle, be reduced from 155 to as few as 31 (80%) without jeopardising the nation’s capacity to produce physicians[6]. In 1913, Flexner became assistant secretary, and later secretary, of the General Education Board at the Rockefeller Foundation[7]. In 1915, Wycliffe Rose and William Welch submitted to this Board their report on the development of schools of public health constructed around a combination of British and German models[8].

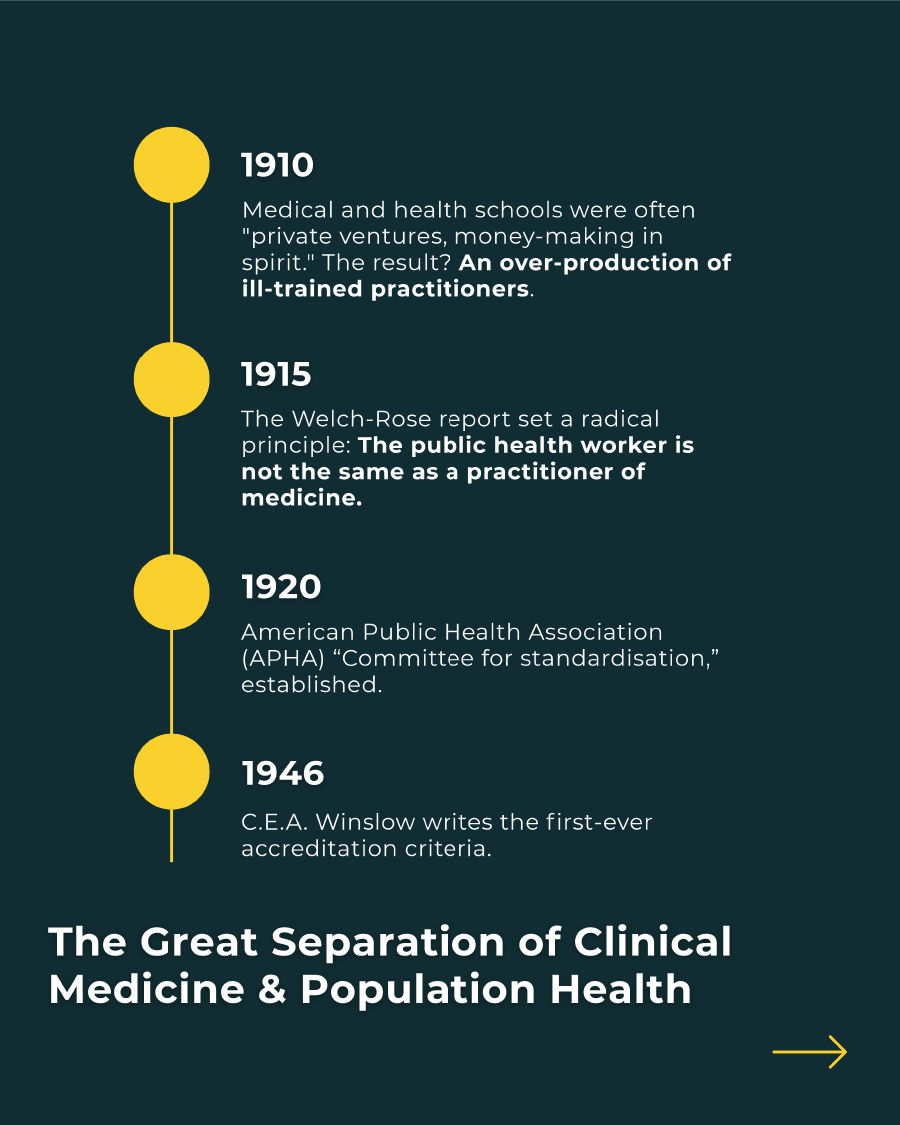

Based on this report, a core principle of the American public health accreditation system was to enforce the separation of public health from medical schools. However, this principle did not reflect either the situation of the British or German systems on which they were based, or indeed many other systems globally[9]. Apart from the notion that “the public health worker was not the same as a practitioner of medicine,” no other rationale for the independence of schools of public health from medical units was provided in the report. Nevertheless, Flexner’s role on the Board and his open antipathy for the vast majority of medical schools provides context for the ‘medical independence’ element within the North American model[10].
Part of Flexner’s concerns were that a lack of standards meant that many medical schools, although called colleges or universities, dealt only with secondary education. This was a criticism that also crossed over to American public health education, “certain institutions give not only the Certificate in Public Health but even the Doctorate in Public Health for a course of a few weeks, while others require a period of almost three years, and it seems most desirable to effect some form of standardization in this field.”[11]
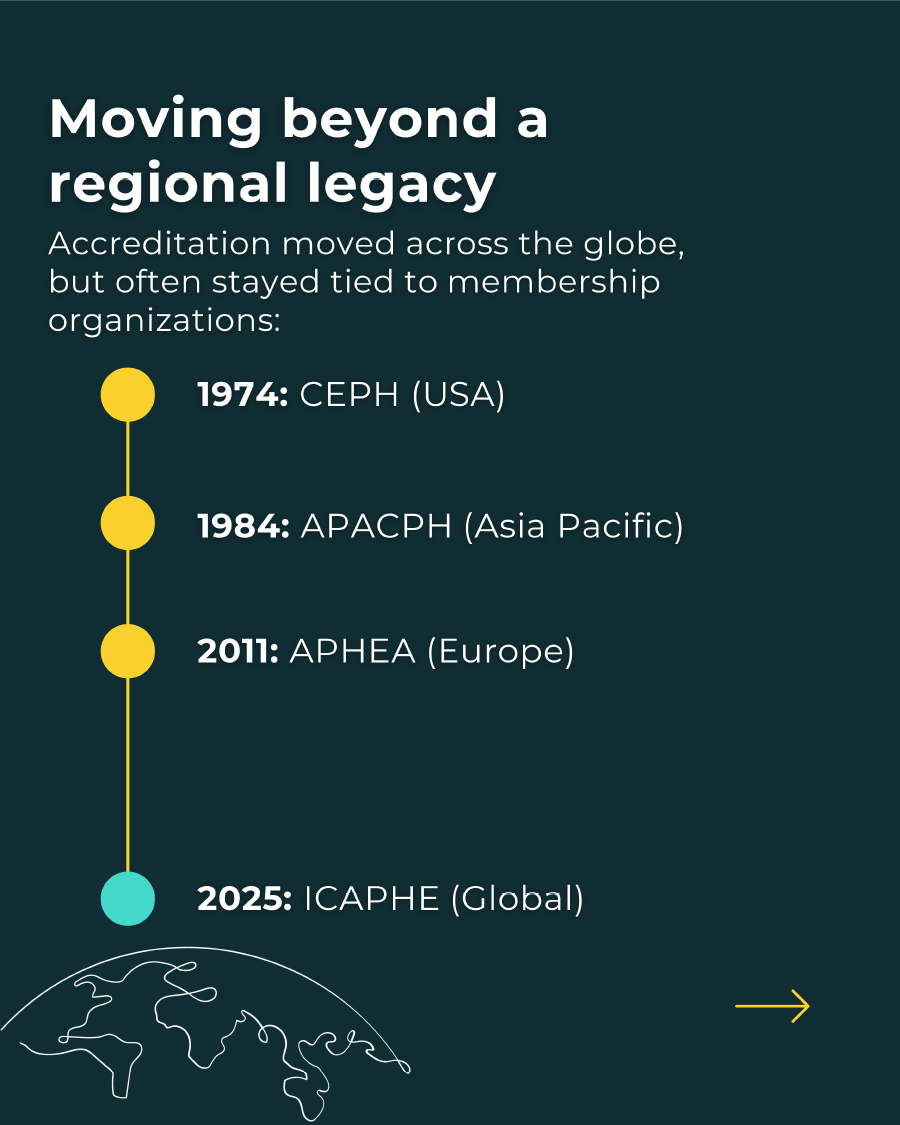
A contemporary of Flexner’s, Charles Edward Amory (CEA) Winslow, argued for schools to focus on community issues and was the original proponent of what is widely perceived as Acheson’s definition of public health[12]. Winslow was later responsible for writing the first public health education accreditation criteria accepted in 1946 by the American Public Health Association (APHA). In 1974, the Council on Education for Public Health (CEPH) was officially established by APHA[13]. Although it was established in 1941 before the advent of accreditation[14], the Association of Schools of Public Health (later renamed the Association of Schools and Programs of Public Health (ASPPH)), restricts membership to those schools and programmes accredited by CEPH[15].
The interconnection or lack of independence of public health accreditation and membership-based organisations can also be seen in other regional accreditation systems, such as the Asia Pacific Academic Consortium for Public Health (APACPH), which was established in 1984. In Europe, accreditation was initiated more recently in 2011 by the Association of Schools of Public Health in the European Region (ASPHER) and other european NGOs. At that time, the Agency for Public Health Education Accreditation in the European Region (APHEA)[16] was solely focussed on the European region[17]. Financial incentives are restricted to members [18].
Despite the gradual expansion to a limited number of schools beyond their regions, these agencies tend to focus on the regions they were established to represent.
ICAPHE views accreditation not only as a quality assurance mechanism but also as a driver of quality improvement in public health education globally. This is why our work supports schools, programmes and training institutes by encouraging shared learning, exchange of experience and the development of a broad, global community of practice. We advance this through collaboration, good-practice sharing and research initiatives.
Our mission is to enhance the quality and impact of global public health education through rigorous accreditation processes, research, collaboration and sharing of good practice. We are committed to empowering educators to excel in a collegial, inclusive and transparent environment.
ICAPHE’s inaugural President, Professor Friday Okonofua stated that: “We have a very lofty mission and set of vision statements. As we say in my country, the taste of the pudding is in the eating. I believe very strongly that we all should work together to ensure that those lofty ideas are not only put on paper but demonstrated to the rest of the world. These include transparency, effectiveness, accountability and anti-corruption.”
Why Norway?
As a foundation established to support the improvement of public health education, driven by a commitment to ethics, equity, sound science and impact, ICAPHE has placed its headquarters in Norway. Our home base is symbolic of many of the ideals we wish to embody as an organisation in our internal operations as well as our many relationships with partners around the globe.
Norway has a longstanding reputation for:
- Being an arbiter for peace and global conflict resolution.
- Being a reliable and substantial contributor to development assistance for health (DAH) through humanitarian aid.
- Global support of sustainable development, climate action, gender equality, food security and health, and human rights.
- A model for transparent governance and low levels of corruption.
- Never being a coloniser.
We support decolonisation and co-equal global partnerships in the public interest. We advocate for change where it is needed to advance our collective wellbeing. We explicitly encourage young people, junior professionals, and those who have not historically had a seat at the table to join us in our work. We commit to a workplace and professional arena that is collegial and does not perpetuate old patterns of domination by an “old guard” acting as a barrier to new voices.
Come join us!
References
[1] Shepard W, Atwater RM, Anderson GW, Bauer W, Defries RD, Godfrey Jr ES, et al. Institutions Accredited by the American Public Health Association to Give the Degree of Master of Public Health (Diploma of Public Health in Canada) for the Academic Year 1946-1947. American Journal of Public Health and the Nations Health. 1946;36(3):244-7. here
[2] Winslow C-EA. The accreditation of North American schools of public health: American Public Health Association; 1953.
[3] Shepard WP. The professionalization of public health. Am J Public Health Nations Health 1948;38(1 Pt 2):145-53 here
[4] Flexner A. I Remember: The Autobiography of Abraham Flexner: Simon and Schuster; 1940. here
[5] Flexner A. Medical education in the United States and Canada. From the Carnegie Foundation for the Advancement of Teaching, Bulletin Number Four, 1910. Bull World Health Organ 2002; 80: 594-602 here
[6] ibid
[7] Abraham Flexner, Past Director, Institute for Advanced Studies here [last accessed 17.12.2025]
[8] Welch W, Rose W. Institute of Hygiene: a report to the General Education Board of Rockefeller foundation. New York: The Rockefeller Foundation; 1915. here
[9] Paccaud F, Weihofen A, Nocera S. Public health education in Europe: old and new challenges. Public Health Reviews. 2011;33(1):66-86.
[10] Elizabeth Fee provides some interesting additional context for this argument when she writes: “Many physicians saw the Rockefeller activities in public health as an assault on their interests as small (medical) businessmen and as an effort to invade their markets. Rose understood this point of view.” See: Fee E. Designing schools of public health for the United States. A history of education in public health: health that mocks the doctors’ rules: Oxford University Press; 1991.
[11] Abbott AC, Boyd M, Bristol LD, Brown WH, Geiger JC, Greeley SA, et al. Standardization of Public Health Training: Report of the Committee of Sixteen. American journal of public health. 1921;11(4):371-5.
[12] Winslow (1920): “Public health is the science and the art of preventing disease, prolonging life, and promoting physical health and efficiency through organized community efforts”
Acheson (1988): “Public health is the science and art of preventing disease, prolonging life and promoting health through the organized efforts of society.”
[14] Rosenstock L, Helsing K, Rimer B. Public health education in the United States: then and now. Public Health Reviews. 2011;33(1):39-65. (page 43 here)
[15] “ASPPH Membership is open to graduate schools and programs of public health that are accredited, or are in the applicant status, by the Council of Education for Public Health (CEPH)” here and here
[16] Federal Public Service Justice, Belgium here
[17] Otok R, Levin I, Sitko S, Flahault A. European Accreditation of Public Health Education. Public Health Reviews. 2011;33(1):30-8. here
[18] Members receive discounted fees see here and here
[19] Internet Archive Book Images, No restrictions, via Wikimedia Commons here